
You wake up and notice it before you’ve even properly opened your eyes: your jaw heavy, your temples tight, a dull headache you can’t place. Or it’s your partner who tells you, half-asleep and half-reproachful: “you’ve been grinding your teeth all night again”. Welcome to the world of bruxism – one of those things we do without realising, and which carries as much confusion as discomfort.
The good news is that science has changed how it understands it a great deal in recent years. The less good news – let’s be honest from the start – is that there’s no magic pill that “cures” it. But there is plenty you can do. Let’s take it step by step.
What is bruxism?
Forget the idea of a “bad habit” or “quirk”. Bruxism is defined as repetitive muscle activity of the jaw, which shows up in two ways: clenching the teeth in a sustained way, or grinding them with back-and-forth movements. What they have in common is that they serve no useful function: you’re not chewing or swallowing – your muscles simply activate on their own.
Daytime and night-time aren’t the same
An international expert consensus (led by Dr Lobbezoo, 2018) drew a distinction that changed everything. There are two different kinds of bruxism, with different causes and management:
| Sleep bruxism | Awake bruxism | |
|---|---|---|
| When | While you sleep | During the day, awake |
| How | More grinding (with noise) | More clenching, in silence |
| Typical trigger | Micro-arousals during sleep | Stress, concentration, tension |
| Who notices it | Your partner, because of the noise | You yourself, if you pay attention |
Telling them apart matters, because what helps with one doesn’t always work for the other.

The shift in thinking: disorder or behaviour?
Here’s one of the most important and least known ideas. Today, in healthy people, bruxism is no longer automatically considered a disease, but rather a behaviour or muscle activity that can have negative consequences… or even be harmless.
- If it’s intense or frequent, it’s a risk factor: tooth wear, muscle pain, problems in the joint.
- In some cases it’s speculated that this night-time muscle activity could play a protective role (for example, helping to keep the airway open or guarding against reflux).
The practical takeaway is liberating: not every case of bruxism needs treatment. You only intervene when it causes real problems.
Why do you clench? Forget the “bad bite”
For decades, the blame fell on poor tooth alignment (“malocclusion”). Current evidence has ruled that out as the main cause. Bruxism is regulated by the central nervous system and is linked to several factors:
- Stress and anxiety. The most powerful trigger, especially of awake bruxism. Tension, frustration, intense concentration… and the jaw clenches.
- Sleep quality. Night-time bruxism is tied to micro-arousals and disorders such as sleep apnoea.
- Lifestyle. Tobacco, alcohol and caffeine increase the risk.
- Certain medications (some antidepressants, for example) can trigger or worsen it.
- Genetics. There’s a familial predisposition.
Did you know…? The mid-afternoon coffee or the drink before bed don’t just cost you sleep: alcohol, caffeine and tobacco are linked to more night-time bruxism. Sometimes, adjusting these habits does more for your jaw than any device.
The clues your body gives
Bruxism leaves traces, and not only on your teeth:
- Tooth wear: flattened, shortened teeth or small fractures (the dentist usually spots it).
- Jaw pain or stiffness, especially on waking.
- A dull headache at the temples in the morning.
- Clicking in the jaw joint (the TMJ) when opening or closing your mouth.
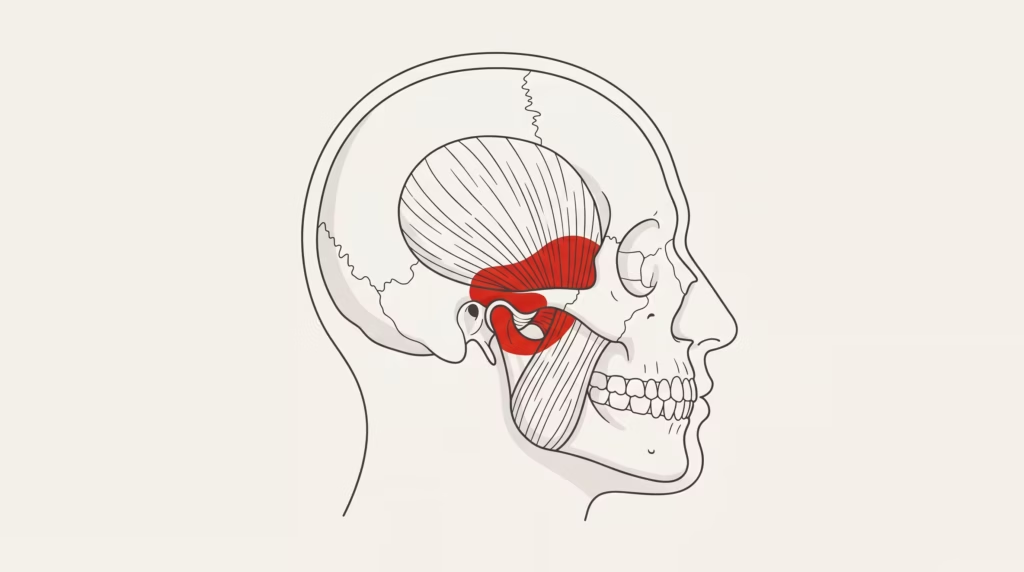
- A more pronounced jaw: the masseter muscle can enlarge and give the face a squarer appearance.
There’s also a close relationship with temporomandibular disorders (TMD): bruxism is a risk factor, and many people with jaw pain clench too. That’s why the neck and the jaw tend to go hand in hand.
How it’s diagnosed
Diagnosis comes in degrees of certainty: possible (what you report), probable (the above plus signs on examination, such as wear or an enlarged muscle) and definite. For sleep bruxism, the reference test is polysomnography, a sleep study that records, among other things, the activity of the chewing muscles. In practice, most cases are managed well without reaching that point.
What actually helps (and what doesn’t “cure”)
Let’s start with the uncomfortable truth: there is no definitive cure for bruxism, because it’s an activity regulated by the brain, not a mechanical fault in the mouth. The aim of treatment is to manage its consequences and reduce how often it happens. What’s supported:
- Occlusal splint. Its well-established job is to protect the teeth from wear and relax the muscles somewhat. Important (and honest): a Cochrane review notes that there isn’t enough evidence that the splint reduces bruxism itself; it protects, but it doesn’t switch off the habit.
- Stress management and sleep hygiene. Given the link with stress and poor sleep, relaxation techniques, mindfulness and cognitive behavioural therapy help to reduce frequency and intensity, especially during the day.
- Biofeedback. Sensors that make you aware of when you’re clenching, so you can learn to let go.
- Botulinum toxin (with caution). It doesn’t prevent bruxism, but it weakens the muscle and reduces force, pain and damage. It’s used “off-label” and the long-term evidence isn’t yet conclusive.
Quick summary — what each thing does
| Tool | What it achieves (and what it doesn’t) |
|---|---|
| Occlusal splint | Protects the teeth; doesn’t “switch off” bruxism |
| Stress management / CBT | Reduces frequency and intensity, especially in the daytime |
| Orofacial physiotherapy | Eases jaw and neck pain |
| Botulinum toxin | Lowers force and damage; cautious, off-label use |
| Adjusting the bite | Not supported as a treatment for bruxism |
The (key) role of physiotherapy

This is where many people don’t realise there’s a route to relief. A physiotherapist specialising in the orofacial area can make a real difference to the muscular symptoms:
- Manual therapy to relax the overloaded chewing muscles (masseter, temporalis and those inside the mouth).
- Treating the neck, because cervical and jaw tension are closely connected: releasing the neck often calms the jaw.
- Exercises for mobility and control to retrain the area.
In fact, the combination of splint + physiotherapy tends to be the most effective approach when there’s pain.
At Clínica QO (Alicante) we work right at that intersection of jaw, neck and tension — with an honest approach: ease the symptoms and teach you to manage them, without selling you an impossible cure. And, as always, we look after you in your own language.
Two myths worth dropping
“It’s cured by adjusting the bite or filing down the teeth.” False. Since occlusion is no longer considered the main cause, invasive and irreversible dental treatments to “cure” bruxism aren’t supported by the evidence.
“If you grind, you definitely need a splint.” False. Treatment is only needed when there are symptoms: pain, significant tooth damage or an impact on your quality of life.
When should you seek help?
Get assessed if you notice persistent pain in the jaw, face or ears; frequent headaches (especially in the morning); visible tooth wear or sensitive/fractured teeth; difficulty or pain opening your mouth; or if your partner complains about the night-time noise. The most effective approach is usually a team one: dentist, physiotherapist and, when stress is the driver, psychological support.
In short
Let’s go back to that morning of a heavy jaw and tight temples. You now know that night-time clenching is no mystery and no punishment: it’s almost always your body releasing tension while you sleep. It can’t be fixed with a miracle device or by filing down teeth, but it can be protected, eased and reduced — by looking after your stress and sleep, releasing the muscles and, if needed, protecting the teeth with a splint.
The key is to stop looking for the switch that turns it off and start working on what really makes a difference. Your jaw, your neck and your rest will feel it.
Do you wake up with a heavy jaw or head? At Clínica QO (Alicante) we assess jaw and neck tension, explain what sets it off and give you a realistic plan to ease it — in your own language.
Frequently asked questions
Can bruxism be cured?
There’s no definitive cure, because it’s an activity regulated by the nervous system, not a fault in the mouth. But it can be managed: protecting the teeth, easing the pain and reducing how often it happens by working on stress and sleep.
Does a splint get rid of bruxism?
It protects the teeth from wear and relaxes the muscles somewhat, but the evidence indicates it doesn’t reduce bruxism itself. It’s a protective tool, not an “off switch” for the habit.
Is it caused by a bad bite?
No. The idea that malocclusion is the main cause has been ruled out. That’s why filing down teeth or irreversible dental treatments aren’t recommended to “cure” it.
What’s its relationship with stress?
Very close, especially with daytime bruxism. Stress, anxiety and tension are among the most powerful triggers, and managing them helps to reduce clenching.
Does physiotherapy help with bruxism?
Yes, especially with jaw and neck pain. Orofacial manual therapy, neck treatment and exercises can ease the symptoms; combined with a splint it’s usually the most effective option.
When should I seek help?
If you have persistent pain in the jaw, face or ears, morning headaches, tooth wear, difficulty opening your mouth or your partner notices night-time grinding.
Sources and reference guides
- Lobbezoo F. et al. — International consensus on the assessment of bruxism (J Oral Rehabil, 2018): https://onlinelibrary.wiley.com/journal/13652842
- Cochrane Library — Occlusal splints for treating sleep bruxism: https://www.cochranelibrary.com/
- Mayo Clinic — Bruxism (teeth grinding): https://www.mayoclinic.org/diseases-conditions/bruxism/symptoms-causes/syc-20356095
- MedlinePlus (NIH) — Bruxism: https://medlineplus.gov/

