The doctor turns the screen toward me, points to a spot between two vertebrae, and utters those two words: “herniated disc.” From that moment on, almost no one hears the rest of the sentence. Their minds have already wandered elsewhere: Will I need surgery? Will I ever be able to hold my son in my arms again? Is this forever?
Take a deep breath. Because what the latest science tells us about herniated discs is much more reassuring than that moment in the doctor’s office might suggest. The vast majority resolve without surgery, and many literally go away on their own. Let’s figure out why—without white coats or complicated jargon.
What exactly is a herniated disc?
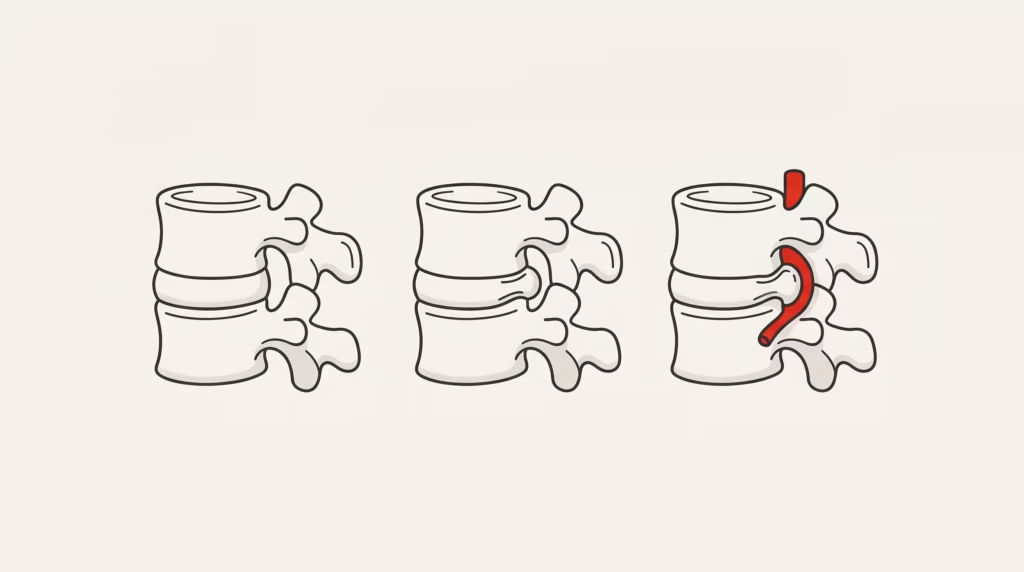
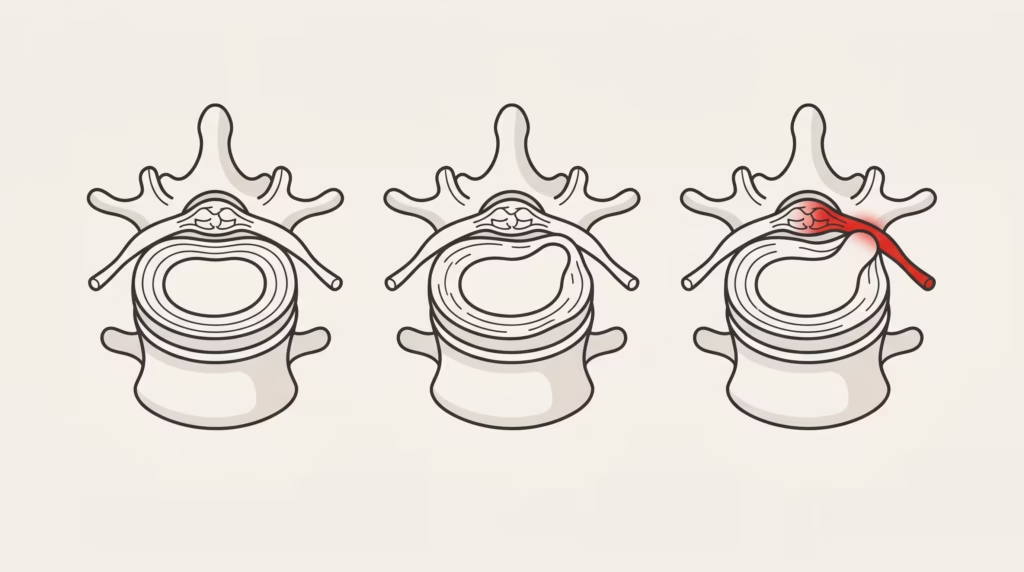
Between every two vertebrae in your spine is a shock absorber: the intervertebral disc. Think of it as a filled doughnut. On the outside, there’s a sturdy ring of cartilage (the annulus fibrosus). On the inside, there’s a gel-like, jam-like center that distributes pressure (the nucleus pulposus).
A hernia occurs when part of that “jam” leaks out through a tear in the ring. And not all hernias are the same:
| Type | What’s up? | Mental image |
|---|---|---|
| Protrusion | The ring bulges, but it doesn’t break | The doughnut loses its shape |
| Extrusion | The ring breaks and the core is revealed | The jam is spilling out |
| Kidnapping | A piece breaks off and comes loose | A piece falls into the canal |
More than 95% of lumbar hernias occur at the bottom two levels (L4-L5 and L5-S1), which bear the most weight. That makes sense: they work the hardest.
Herniated Disc and Sciatica: Similar but Not the Same
🎬 Promotional video
This is the most common misunderstanding, so it’s worth setting the record straight once and for all:
- A herniated disc is the anatomical cause: the injury to the disc.
- Sciatica is the most well-known symptom: pain that radiates down the leg when the herniated disc rubs against or irritates a nerve root.
You can have a herniated disc without experiencing sciatica. And you can have sciatica for other reasons. But when they occur together, the underlying problem is nerve irritation, not “a bone out of place.” (If you’re mainly concerned about pain running down your leg, we have an article dedicated solely to sciatica.)

Why Me? Causes and Risk Factors

A hernia is rarely caused by a single wrong move. It’s usually the straw that breaks the camel’s back after years of strain. What fills that camel’s back:
- Age and natural wear and tear. This is the main factor: over time, the disc loses water and elasticity.
- Genetics. There are families with factory-made discs of “lower quality.”
- A sedentary lifestyle. Less muscle to support the spine = more pressure on the disc.
- Tobacco. It reduces the amount of oxygen reaching the disc and accelerates its aging.
- Repeated strain and twisting, as well as being overweight, which add up to kilos of pressure.
Did you know…? Smoking doesn’t just affect your lungs: it reduces blood flow to the intervertebral disc and is considered a real risk factor for disc degeneration. That’s one more—and little-known—reason to quit.
The fact that changes everything: most hernias heal on their own
If you take away just one idea from this entire article, let it be this one. It’s solidly backed by evidence and dispels fear in one fell swoop.
First: Many herniated discs don’t cause pain. When people without any back pain have had MRIs, a very high percentage were found to have herniated or bulging discs without even knowing it. Finding a herniated disc on an image doesn’t automatically mean it’s the cause of your pain.
Second, and even better: many hernias resolve on their own. When the nucleus protrudes into the canal, your immune system treats it as an intruder and gradually “clears” it away. A 2024 systematic review found that about 76% of lumbar hernias treated without surgery resolved spontaneously. And here’s the paradox: larger hernias (extrusions and sequestrations) tend to resolve on their own more readily, because they trigger a more intense inflammatory response.
That process can take anywhere from 3 to 12 months, but pain relief almost always comes much sooner. Your body is simply on your side.
The diagnosis: Treat the patient, not the MRI
This is where a dose of clinical common sense comes in handy. The diagnosis is based primarily on what you describe and on the physical exam: where it hurts, how far down the pain extends, which movements trigger it, and how your strength, reflexes, and sensation are.
The MRI confirms the hernia, yes, but with one major caveat: since so many healthy people have hernias, a finding on the scan only matters if it matches your symptoms. Ordering MRIs right away, without a clear indication, usually causes more fear than it provides solutions. It’s a good sign if your doctor doesn’t rush to order tests—it means they know what they’re doing.
Warning Signs: When to Go to the Emergency Room
The vast majority of hernias are not emergencies. However, there is a rare and serious condition— cauda equina syndrome—in which a very large hernia suddenly compresses the bundle of nerves at the end of the spinal cord. It requires immediate attention.
⚠️ Go to the emergency room immediately if you notice:
- Loss of bladder or bowel control (leaks or inability to urinate).
- Numbness in the genital area, perianal area, or inner thighs (“saddle anesthesia”).
- Significant weakness or rapidly worsening weakness in both legs.
- Sudden loss of sexual function.
A “drooping foot” that is clearly getting worse also warrants immediate medical attention. These cases are rare, but it’s important to recognize them.
Treatment: The conservative approach is the primary one
Forget about complete bed rest: it’s a thing of the past and can slow down your recovery. The NICE guideline (NG59) recommends an active approach, which is exactly what the evidence supports.
- Stay active. Getting on with your life as much as possible is better than staying in bed.
- Exercise and physical therapy. The cornerstone of treatment—motor control and strengthening exercises, ideally prescribed by a professional—reduces pain and disability.
- Manual therapy (mobilization, manipulation), combined with exercise—not instead of it.
- On-demand pain relief (anti-inflammatory drugs) at the minimum effective dose and for the shortest possible time.
Regarding chiropractic and osteopathy: they primarily use manual therapy, and their effectiveness is similar to that of other forms of manual therapy when used as part of an active treatment plan. To be honest, it’s best to be clear: they help as part of a comprehensive treatment plan, but they’re not a magic wand. What lacks solid evidence is the use of traction or passive electrotherapy as a primary treatment.
Quick Summary — What Helps and What to Avoid
| Yes, it helps | Best to avoid |
|---|---|
| Stay within reasonable limits | Complete bed rest |
| Guided and Progressive Exercise | Search for “the magic pose” |
| Manual therapy + exercise | Traction/electrotherapy as a foundation |
| Patience (weeks, not days) | Rushing into surgery without trying a conservative approach first |
When are injections or surgery considered?
When conservative treatment, when properly administered, does not work after several weeks, or if there is significant neurological impairment, other options are considered.
Epidural corticosteroid injections can relieve pain in the short term (less than 3 months) by reducing inflammation around the nerve. They do not change the course of the herniation, but they can “buy time” to allow for rehabilitation with less pain.
Surgery —typically a microdiscectomy, which removes only the fragment compressing the nerve—is reserved for: cauda equina syndrome (urgent), progressive or severe neurological deficits, or incapacitating leg pain that does not respond after 6–12 weeks of appropriate treatment. An important point: surgery is much more effective at relieving leg pain than lower back pain itself.
Outlook: Realistic and Hopeful
Let’s wrap up with some reassuring statistics. The natural course of a lumbar disc herniation is overwhelmingly favorable: about 30% of patients show improvement within the first 6 weeks, and up to 60% within 6 months with conservative treatment. In the long term, patients who undergo surgery and those who do not often end up at a similar point; when properly indicated, surgery primarily provides faster relief from leg pain.
In summary
Let’s go back to that moment in the doctor’s office—to the screen swiveling and the two words that sent a chill down your spine. Now you know what that initial shock kept you from seeing: a herniated disc isn’t a death sentence. It’s a sign that your back needs attention and smart movement. In most cases, time, exercise, and good support do the trick—and your own body, by reabsorbing the herniation, plays a huge part.
If you live in fear of moving because of a hernia, that fear often does more harm than the hernia itself. Regaining confidence is part of the treatment.
Are you worried about a herniated disc? At Clínica QO (Alicante), we assess your case without causing undue alarm, explain what your symptoms mean, and design a personalized treatment plan—in your language.
Frequently Asked Questions
Does a herniated disc heal on its own?
In many cases, yes. Most improve with conservative treatment, and a significant number of hernias resolve spontaneously within 3 to 12 months, especially the larger ones.
Does having a hernia mean I’ll need surgery?
No. Surgery is reserved for a small number of patients: those with warning signs, progressive neurological deficits, or disabling pain that does not subside after weeks of well-managed conservative treatment.
Can I exercise with a herniated disc?
Yes, and in fact, it’s part of the treatment. Prolonged rest is counterproductive. The ideal approach is a progressive program guided by a professional and tailored to your stage of recovery and your symptoms.
Do I need an MRI to treat my hernia?
Not always. The diagnosis is based primarily on clinical findings. An MRI is only useful if its findings match your symptoms, because many people without pain also have hernias.
Is a herniated disc the same thing as sciatica?
No. A herniated disc is the cause; sciatica is the pain that radiates down the leg when a nerve is irritated. A herniated disc can cause sciatica, but the two terms are not synonymous.
How long does it take to get better?
There is usually a noticeable improvement within a few weeks. About 30% improvement is seen in the first 6 weeks, and up to 60% at 6 months with conservative treatment.
Sources and Reference Guides
- NICE — Low Back Pain and Sciatica in People Over 16 (NG59): https://www.nice.org.uk/guidance/ng59
- Cochrane Library — reviews on epidural injections, traction, and manual therapy: https://www.cochranelibrary.com/
- Systematic review on spontaneous resolution of lumbar disc herniation (2024), via PubMed/NIH: https://pubmed.ncbi.nlm.nih.gov/
- MedlinePlus (NIH) — Herniated Disc: https://medlineplus.gov/spanish/herniateddisk.html



