A mother watches her daughter try on a dress and notices something: one shoulder seems higher than the other, and the waist isn’t quite symmetrical. Or maybe it’s you, a few years older now, and your lower back aches every afternoon while someone mentions, almost in passing, the word “scoliosis.” In both cases, the same flood of doubts sets in: Is it serious? Did I do something wrong? Can it be corrected?
Let’s shed some light on this, because few spinal conditions are surrounded by so many myths. Scoliosis isn’t what many people think it is—and understanding what it really is is the first step toward making good decisions.
What is scoliosis (and what is it NOT)?
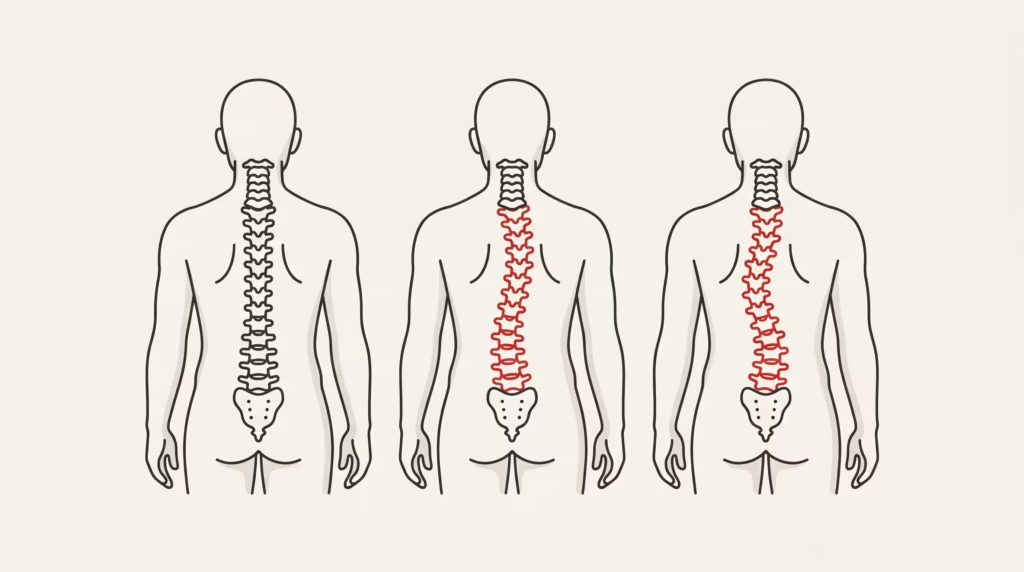
Scoliosis is a three-dimensional curvature of the spine: when viewed from the front on an X-ray, instead of a straight line, it forms an “S” or a “C.” To be diagnosed as scoliosis, that curve must measure at least 10 degrees (the so-called “Cobb angle”). And there’s a key detail: the vertebrae not only tilt but also rotate around their own axes.
Here’s the first myth we need to debunk: scoliosis is not “bad posture.” It’s not caused by sitting crooked, nor can it be corrected by “sitting up straight.” It’s a structural condition of the spine, and that completely changes how it’s treated.
Not all cases of scoliosis are the same
🎬 Promotional video
Depending on their origin, there are several types:
| Type | When it appears | Details |
|---|---|---|
| Idiopathic | Especially during adolescence | The most common (>80%); exact cause unknown |
| Congenital | From birth | Due to spinal malformations |
| Neuromuscular | Associated with another disease | Cerebral palsy, muscular dystrophy… |
| Adult-Onset Degenerative Disease | After 50, “de novo” | Due to asymmetric wear on discs and joints |
The main focus is on idiopathic adolescent growth spurt: it occurs during the growth spurt, and although “idiopathic” may sound alarming, it simply means that there is no single identifiable cause.

Why does it appear? Neither backpacks nor sports
It’s time to debunk the most widespread myths, because they cause a lot of unnecessary guilt, especially within families.
Idiopathic scoliosis is not caused by heavy backpacks, sleeping on one side, playing a specific sport, or sitting in an improper position. It does, however, have a strong genetic component: it is common for several cases to occur within the same family. A heavy backpack can cause back pain, true, but it does not lead to the structural deformity associated with scoliosis.
Did you know…? Mild scoliosis occurs with almost equal frequency in boys and girls, but girls are at much greater risk of the condition progressing: in cases of scoliosis exceeding 40 degrees, the ratio can be as high as 7 girls for every boy.
How is it detected? Signs and the Adams test
In children and adolescents, scoliosis doesn’t usually cause pain, which is why it often goes unnoticed. The signs are visual:
- One shoulder is higher than the other.
- A more pronounced shoulder blade.
- Uneven waist or hips.
- The trunk is slightly shifted to one side.
The most well-known test is simple, and you may have seen it in school: the Adams test. When you lean forward with your legs together and your arms hanging down, if you have scoliosis, a small “hump” appears on one side of your back—this is the rotation of the ribs becoming visible.
In adults, the picture is different: here, the main symptom is usually back pain and stiffness, sometimes with pain radiating down the leg.
The Diagnosis: The Cobb Angle

Confirmation comes from an X-ray of the entire spine, in which the specialist measures the Cobb angle. That number determines the severity and guides everything else:
- Mild: 10–25 degrees.
- Moderate: 25–45 degrees.
- Severe: over 45–50 degrees.
It’s not just a technical quirk: the degree of the curve, along with how much the patient still has left to grow, is what determines the treatment.
Treatment: depends on the curve and growth
There is no single treatment for scoliosis; rather, the appropriate treatment varies from case to case. The decision hinges on two questions: How severe is the curve? And how much growth remains?
- Note. For mild curvatures, or in patients who have already finished growing, the best approach is usually to monitor the condition with periodic checkups. Not over-treating is also good medicine.
- Brace (orthosis). For moderate curves in growing patients, this is the treatment of choice, backed by solid evidence: the BrAIST study (published in the New England Journal of Medicine in 2013) demonstrated that bracing clearly reduces the risk of the curve progressing to the point where surgery is necessary. Its success depends heavily on how many hours a day it is worn. Keep this important point in mind: the goal of the brace is not to straighten the curve, but to slow its progression during growth.
- Surgery (arthrodesis). It is reserved for severe curves (greater than 45–50°) that continue to progress. It corrects and stabilizes the spine by fusing vertebrae.
The Role of Exercise: Specific Physical Therapy (SPT)
This is where a very interesting tool comes into play: specific physical therapy exercises for scoliosis (PSSE), notably the Schroth method. These are not “generic exercises”; they are programs designed to address the curve in three dimensions.
The guidelines from the leading international organization (SOSORT) recommend them as a first step for mild curvatures and as a complement to a brace to improve posture and compliance. The evidence is promising—they can help slow progression and improve quality of life—although rigorous reviews, such as those by Cochrane, remind us that more high-quality research is still needed to draw definitive conclusions. Let’s be honest: they help, but they’re not magic.
What DOESN’T flatten the curve (let’s be clear)
This part is uncomfortable but necessary, because there’s a lot of exaggerated hype out there. There is no solid evidence that chiropractic or osteopathic care can correct or halt structural scoliosis. They can help manage associated back pain, improve mobility, or treat nonstructural postural imbalances—and that is valuable—but presenting them as a “cure” for scoliosis is not scientifically sound.
To put it bluntly: be wary of anyone who guarantees they can correct a structural curvature through manual therapy sessions. It’s one thing to relieve discomfort and improve your daily life; it’s quite another to correct the deformity.
Quick Overview — What Each Feature Does
| Objective | Tool with a backrest |
|---|---|
| Slowing the Rate of Growth | Corset (moderate curves) |
| Working on Your Curve Through Exercise | PSSE / Schroth (supplement) |
| Correcting Severe Curves | Surgery (arthrodesis) |
| Relieve associated pain | Physical therapy, exercise, manual therapy |
Scoliosis in Adults: The Focus Is on Pain
In adulthood, the priority is rarely the angle of the curve: it is to live well and without pain. Initial treatment is almost always conservative—physical therapy and exercise to strengthen the core and improve posture, as-needed pain relief, and, in select cases, injections for radiating pain. Surgery is reserved for disabling pain or neurological deficits that do not respond to other measures.
In summary
Let’s go back to that scene by the mirror, to the shoulder that was slightly higher, and to the word that set off all the alarms. Now you see it in a different light: scoliosis isn’t anyone’s fault; it wasn’t caused by a backpack or poor posture, and it’s rarely the catastrophe that the initial scare suggests. Most mild curves do not progress or cause problems; those that do have treatments backed by solid evidence, depending on age and severity.
The most important thing is not to go to extremes: neither to downplay a growth curve that’s rising during adolescence nor to overreact to a slight deviation that simply requires monitoring. Between fear and false hope lies a sensible path, and it almost always involves a thorough evaluation.
Do you have concerns about scoliosis—yours or your child’s? At Clínica QO (Alicante), we assess your curve, explain what it means without causing alarm, and design an honest plan—including exercise, follow-up, and referrals when necessary—in your language.
Frequently Asked Questions
Can scoliosis be corrected by standing up straight or maintaining good posture?
No. Scoliosis is a structural curvature of the spine, not poor posture. “Standing up straight” does not correct it, although working on your posture and strengthening your muscles can help with pain and function.
Is it caused by heavy backpacks?
No. Idiopathic scoliosis is not caused by backpacks, sports, or sleeping on one side. It has a strong genetic component. A heavy backpack can cause back pain, but it does not cause the deformity.
Does a corset straighten the spine?
That is not its purpose. In growing patients with moderate curves, the brace serves to slow the progression of the curve, and its effectiveness in preventing surgery is well supported by the evidence.
Is exercise worth it?
Yes, as a supplement. Specific exercises for scoliosis (PSSE, such as the Schroth method) can help slow the progression of the condition and improve quality of life, although research is still ongoing to determine the best protocol.
Can chiropractic or osteopathy cure scoliosis?
There is no solid evidence that they correct structural scoliosis. They may help with pain or mobility, but they should not be presented as a cure for the curve.
Is surgery always performed for adult scoliosis?
No. In adults, the focus is on pain and quality of life, and most cases are managed conservatively with physical therapy and exercise. Surgery is reserved for severe cases that do not respond to treatment.
Sources and Reference Guides
- SOSORT — Guidelines for the orthopedic and rehabilitation treatment of idiopathic scoliosis: https://www.sosort.org/
- Weinstein SL et al. — Effects of Bracing in Adolescent Idiopathic Scoliosis (BrAIST), NEJM 2013: https://www.nejm.org/doi/full/10.1056/NEJMoa1307337
- Cochrane Library — exercise/PSSE for adolescent idiopathic scoliosis: https://www.cochranelibrary.com/
- Scoliosis Research Society (SRS): https://www.srs.org/